Diabetes Found To Be A Significant Risk Factor For Dementia



London based Alzheimer’s Disease International: The International Federation of Alzheimer’s Disease and Related Disorders Societies, Inc., supported by a grant from Bupa, has released its comprehensive and thoroughgoing World Alzheimer Report 2014: Dementia and Risk Reduction An Analysis Of Protective And Modifiable Factors. The paper reviews a wide range of research pertaining to Alzheimer’s Disease (AD) and other forms of dementia worldwide, noting that dementia, including AD, remains one of the biggest global public health challenges facing our generation.
Dementia is caused by a constellation of progressive illnesses and health/lifestyle conditions that affect memory, thinking, behaviour and the ability to perform everyday activities. It has an insidious onset typically characterized by an initial subtle decline in one or more cognitive functions including memory and reasoning. Dementia mainly affects older people but two to 10% of all cases are estimated to start before the age of 65 years. After this, prevalence doubles with every five year increment in age. Dementia is one of the main causes of dependence and disability at older ages.
The report has been produced to inform health promotion and disease prevention strategies. The coauthors have examined critically the evidence for the existence of modifiable risk factors for dementia, focusing in particular on sets of potential modifiable risk factors in four key domains; developmental, psychological and psychosocial, lifestyle and cardiovascular risk factors.
They note that although brain damage accumulates and cognitive function declines progressively with age, dementia is not a normal part of aging and most older adults will never develop the disease up to the time of death. However, marked inter-individual differences in cognitive health in late-life are observed at a population-level. While these differences may in part be a function of the level of exposure to a number of factors across the entire life course and are usually termed risk or protective, depending on whether, in general, they are associated with an increased or reduced future likelihood of cognitive impairment and dementia in populations.
Because there are no established diagnostic biomarkers of dementia-related brain damage, and because the mechanisms that link this damage to the expression of dementia symptoms are not fully understood, the coauthors note that prevention of dementia is commonly conceived as delay of the clinical onset of the disease rather than a slowing or avoidance of development of the underlying neuropathology. Similar to other chronic diseases, they say primary prevention of dementia corresponds, ideally, to delay until death of symptomatic onset, or, failing that, a delaying or deferring of onset to older ages than that at which it would otherwise have occurred. They observe that an average five year delay in age of onset would tend to reduce population dementia prevalence by 50 percent, hence greatly reducing its impact in society in general.
[adrotate group=”3″]
The coauthors observe that an estimated 44 million people are currently living with dementia worldwide, a metric that is projected to almost double by 2030 and more than triple by 2050, and that the global cost of dementia was estimated in 2010 at US $604 billion, and expected to rise commensurately/
They note that given this staggering epidemic scale, and with no known cure, its crucial that effort to be focused on reducing the risk and/or delaying the onset of developing dementias, and maintain that Alzheimers disease and other forms of dementia must become a national and international public health priority,and that governments must develop adequate strategies to deal with the epidemic holistically — including tackling both reduction in risk for future generations, and adequately caring for people living with the condition and supporting their friends and family.
A spectrum of possible and likely risk factors for development of dementia are analyzed and discussed in the paper, one being that Diabetes in late-life (and probably in midlife) is associated with an increased risk of all forms of dementia, particularly vascular dementia.
Diabetes & Dementia
The chapter addressing diabetes is coauthored by Prof. Jose A. Luchsinger of the Columbia University Medical Center, New York, Prof. Emiliano Albanese of the University of Geneva, Switzerland, and Prof Martin Prince of The Global Observatory for Aging and Dementia Care, Kings College, London, who note that Type 2 diabetes is one of the more common chronic conditions globally, pointing out that in the United States alone, a third of the adult population has either type 2 diabetes or its antecedent, pre-diabetes.
They observe that prevalence of diabetes increases sharply with age, from 2.4 percent in those aged 20-39 years to 21.6 percent among people aged 65 years and over, with the trend in recent years being that the largest increases have occurred in the oldest age groups, and general trend, in both developed and developing countries, towards an increasing prevalence of pre-diabetes and diabetes, linked to increases in obesity due to a sedentary life-style The high prevalence of diabetes makes it potentially one of the most important modifiable risk factors for dementia.
For example, the paper’s coauthors point out that in contrast to type 1 diabetes, most cases of type 2 diabetes are brought on by lifestyle factors and thus to a large degree preventable, and that regular exercise exercise, losing weight, cutting fat and sugars in the diet, reducing alcohol consumption and stopping or avoiding smoking should all reduce risk. Diabetes, once developed, can be treated with diet, oral hypoglycaemic drugs or insulin.
The researchers suggest several possible mechanisms by which diabetes may act to increase the risk of dementia and AD, but note that there is no clear consensus as yet on the mechanism or mechanisms that might support a causal association, and while diabetes is an important component of the metabolic syndrome, association of the metabolic syndrome with dementia is inconsistent, with some studies indicating a specific association with the diabetes component alone. Insulin resistance is an antecedent and correlate of diabetes, and thought by some to be a central mechanism in the metabolic syndrome, but few studies have demonstrated an association with dementia.
Drs. Luchsinger, Albanese, and Prince reviewed several studies that have examined the relationship between diabetes and dementia mechanisms, particularly surrogate markers of Alzheimer’s Disease, and found conflicting results. They say an association between diabetes and dementia has been shown across countries, continents, and ethnic groups, with the most disadvantaged demographic groups, such as minorities in the United States, indicated to be most heavily impacted by the association between diabetes and dementia. However, they observe that and ethnic disparities in diabetes prevalence may account for some of the unequal distribution of incident cognitive impairment between ethnicities, and it remains unclear whether prevention, or more effective treatment of diabetes can prevent dementia.
They cite two recent meta-analyses, of 17 longitudinal studies (1966-2010) published in 2012 and of 28 longitudinal studies (up to Jan 2012) published in 2013, concurring that diabetes is associated with incident AD, VD, and dementia in general, but maintain that these findings are are problematic — first and foremost because only nine studies are common between the two reviews, which is partly explained by duplicate and overlapping publications. However, they note that there are also some apparent omissions and limitations; both reviews included studies that used health service or hospital registers to ascertain dementia outcome, and some which had used the same approach to identify diabetes exposure. Neither review makes a clear distinction between midlife and late-life exposure to diabetes. Most critically, the way in which the diabetes exposure was ascertained was not classified.
Consequently, the researchers carried out a new review, merging studies from both recent reviews, checking carefully for duplication, and adding any further eligible studies identified in the course of the new search. They applied the same inclusion and exclusion criteria as the previous reviews (prospective or historical population-based cohort studies reporting on the association of diabetes with any dementia (AnyDem), Alzheimers disease (AD) or vascular dementia (VaD)), but excluded health record linkage studies other than for narrative description and discussion. They found 19 eligible studies, and stratified their meta-analyses by the stage in the life course at which exposure had been ascertained (midlife or late- life), and as a sensitivity analysis, restricted inclusion to those studies in which undiagnosed as well as diagnosed diabetes had been ascertained.
They report that evidence reviewed confirms a particularly strong and consistent association between diabetes in late-life and the subsequent onset of dementia. — in contrast to the pattern observed for hypertension, obesity and dyslipidaemia, where increased risk, if it exists, is only apparent for midlife exposures.
Drs. Luchsinger, Albanese, and Prince maintain that clearly this may have important implications for prevention. However, in contrast to other CVRF, relatively few randomized controlled trials have been conducted to assess if improved diabetes control results in a lower incidence of dementia, although evidence from health record linkage studies suggests that diabetes in midlife may have an equivalent or even greater effect, and it may be that the duration of diabetes is an important risk determinant.
The coauthors contend that primary prevention of diabetes should therefore be targeted, since diabetes seems to be a much stronger risk factor for vascular dementia than for Alzheimers disease, and cerebrovascular disease is likely to be an important mediating mechanism. However, they caution that other causal mechanisms may also be involved, including direct influences on AD neuropathological processes, and it remains possible that processes or genetic predispositions that underlie both diabetes and AD, could explain a link that is not causal, and it’s also possible that diabetes decreases brain resilience, but does not directly cause Alzheimer’s Disease.
However, Diabetes in late-life (and probably in midlife) is found to be associated with increased risk of all forms of dementia, particularly vascular dementia, and the robust associations of diabetes and hypertension with dementia give much cause for optimism that a significant proportion of the incidence of dementia could be prevented through more effective prevention, detection and control of these diseases, which the coauthors say is currently sub-optimal in all world regions, and particularly in low and middle income countries where the prevalence of these exposures is increasing due to lifestyle change.
Drs. Luchsinger, Albanese, and Prince project that improved understanding of causal mechanisms will help to shape diabetes treatment and prevention strategies to prevent dementia, and observe that is also important to know whether Alzheimer’s based dementia treatment and prevention strategies could also be useful in people with diabetes, or whether other strategies should be pursued. In the meantime, the rising and overlapping epidemics of diabetes and dementia mean that older people with diabetes are increasingly likely to have cognitive impairment, affecting their self-care, and potentially resulting in more adverse dementia and diabetes outcomes. This will pose a challenge for healthcare systems worldwide.
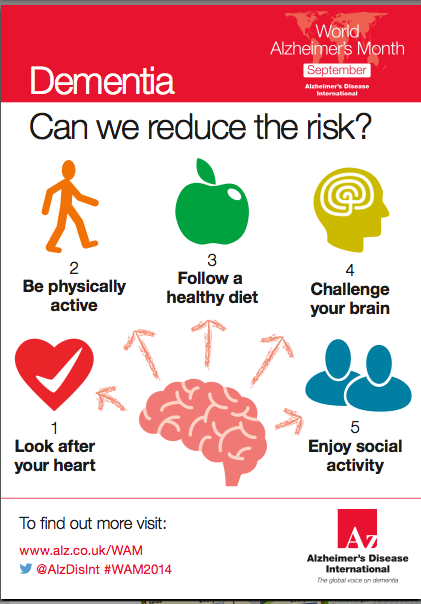
Following the advice of this infographic can help lessen that growing burden.
Alzheimers Disease International: The International Federation of Alzheimers Disease and Related Disorders Societies, Inc. is based in London and is registered as a non- profit organization in the USA, incorporated in Illinois, and is a 501(c)(3) not-for-profit organization. ADI was founded in 1984 and has been in official relations with the World Health Organization since 1996. Each of ADI’s 84 members is a non-profit Alzheimer association supporting people with dementia and their families. ADI’s vision is an improved quality of life for people with dementia and their families throughout the world. ADI aims to make dementia a global health priority, to build and strengthen Alzheimer associations, and to raise awareness about dementia worldwide.
For more information, visit:
https://www.alz.co.uk
Bupa is a leading international healthcare group, offering health insurance and medical subscription products, run care homes, retirement villages, hospitals, primary care centres and dental clinics. We also provide workplace health services, home healthcare, health assessments and long-term condition management services.
Bupa has over 22m customers in 190 countries, and employs more than 70,000 people, principally in the UK, Australia, Spain, Poland, New Zealand and Chile, as well as Saudi Arabia, Hong Kong, India, Thailand, and the USA. With no shareholders, Bupa invests its profits to provide more and better healthcare and fulfil its purpose.
During any given year, Bupa cares for more than 65,000 people in nearly 460 care homes and retirement villages in the UK, Spain, Australia, New Zealand and Poland, and is the leading international provider of specialist dementia care. Of Bupa’a care home residents, around three quarters have dementia.
For more information, visit
https://www.bupa.com
Sources:
Alzheimers Disease International
Bupa
Infographic
Alzheimers Disease International